
Osmosis & Diffusion labs
Background: We first learn about diffusion and osmosis
Here is a lab from sciencespot.net
By Sue Remshak, Lake Bluff Middle School, Lake Bluff, IL
Activity I
During this activity students investigate the concepts of osmosis and diffusion using eggs. To prepare:
* measure and record the circumference of the raw egg
* measure mass.
* Place the egg in a beaker filled with white vinegar.
* Students to record their observations.
* Store the eggs in a refrigerator for 24 hours.
* View again and record their observations.
* Return the egg to the refrigerator for another 24 hours.
* View again and record their observations
For the worksheet click here – Student worksheet
What is all this about?
A chemical reaction occurs between the vinegar and the calcium carbonate in the egg shell. The bubbles of carbon dioxide that form on the egg and rise to the surface are evidence of this reaction.

Photo from Moving Mountains Daily
photo above from The Embarrassed Egg and Osmosis
The shell dissolves in the vinegar and leaves a film on the surface of the vinegar.
However, the membrane remains on the egg. The size of the egg increases because of the movement of water in the vinegar through the cell membrane.
Since water moves from an area of high concentration to an area of low concentration, this process is called osmosis. Obviously, none of the materials on the inside of the egg are able to pass through the membrane.
Activity II
Materials: water, blue water (food coloring in water), molasses, and corn syrup.
First, have the students determine the mass of the egg and record it in the table.
They should pour 150 ml of each substance into its own beaker.
Add the eggs and store in a refrigerator for 24 hours.
After 24 hours, remove the eggs from the beakers and record their observations.
Students should record the volume of liquid in the beaker as well as the mass of the egg.
Use a toothpick to pop the egg membrane and record their observations. Be sure to have paper towels handy as some eggs may squirt!)
What is all this about?
The egg in plain water and blue water will become slightly larger because water will pass into egg through the membrane by the process of osmosis. There will be blue food coloring in the egg from the blue water since both water and food coloring can pass through the membrane.
The egg in corn syrup and molasses will decrease in size because water from inside the egg flow through the membrane into the syrup or molasses. It moves from a higher concentration inside the egg to a lower concentration in the corn syrup.
This is called osmosis. The corn syrup and molasses molecules are too large to pass through the membrane. Observant students will not only notice an increase of volume in the beaker, but they will also see a thin layer of water resting on top of the syrup and molasses.
Activity III
To illustrate the concept of diffusion, add a drop or two of extract (vanilla, bubble gum, lemon, or cinnamon) into a deflated balloon.
Blow up the balloon, tie it off, and place inside a shoe box. To make sure the lid stays on the box, use masking tape to secure it.
During class, ask students to life one end of the shoe box lid and smell the contents. Their eyes should remain closed when they do this.
Ask each student to reveal what they smelled. Show the class what was inside the box and instruct them to draw a picture and record their observations.
Challenge students to write an explanation (using the correct vocabulary) of why the box smells like the scent when it was only put inside the balloon.
What is all this about?
The shoe box smelled of the scent even though it was only placed on the inside of the balloon due to the process of diffusion. Every balloon has microscopic holes in its surface. The vapors were able to pass through the membrane from an area of high concentration to an area of low concentration. However, the liquid scent molecules were too large to pass through the membrane.
Another way to illustrate osmosis and diffusion is using a tea bag and some water. During class, place a tea bag in a beaker of warm water. Allow time for students to record their observations. Challenge them to write an explanation using the correct vocabulary.
Articles on waves
What are waves? They are a repeated disturbance that spreads out, and transfers energy as it moves forwards.


When we study the physics of waves, we cover these topics:
Interference and superposition
Waves in 2 dimensions, and refraction
What is sound? How do we hear it?
Actually see the speed of sound at a Queen concert
Sources of sound: String instruments, harmonics, wind instruments, quality of sound
Diffraction: The way that waves spread around an obstacle
MCAS Physics exam: sample wave problems
when time allows we may address these fun related topics:
How do record players and vinyl LPs work?
Anomalous sounds (sound “mirages”?!)
Sonar, echolocation, and ultrasound
Why pianos are never in tune: Math and Physics.
Facts and Fiction of the Schumann Resonance

And in doing so we cover these learning standards:
Massachusetts Science and Technology/Engineering Curriculum Framework
HS-PS4-1. Use mathematical representations to support a claim regarding relationships among the frequency, wavelength, and speed of waves traveling within various media. Recognize that electromagnetic waves can travel through empty space (without a medium) as compared to mechanical waves that require a medium
SAT subject test in Physics: Waves and optics
• General wave properties, such as wave speed, frequency, wavelength, superposition, standing wave diffraction, and Doppler effect
• Reflection and refraction, such as Snell’s law and changes in wavelength and speed
• Ray optics, such as image formation using pinholes, mirrors, and lenses
• Physical optics, such as single-slit diffraction, double-slit interference, polarization, and color
When Children Say They’re Trans
By Jesse Singal, The Atlantic, July/August 2018

image from Between the (Gender) Lines: the Science of Transgender Identity, Science In The News, Harvard U.
Claire is a 14-year-old girl with short auburn hair and a broad smile. She lives outside Philadelphia with her mother and father, both professional scientists. Claire can come across as an introvert, but she quickly opens up, and what seemed like shyness reveals itself to be quiet self-assuredness. Like many kids her age, she is a bit overscheduled. During the course of the evening I spent with Claire and her mother, Heather—these aren’t their real names—theater, guitar, and track tryouts all came up. We also discussed the fact that, until recently, she wasn’t certain she was a girl.
Sixth grade had been difficult for her. She’d struggled to make friends and experienced both anxiety and depression. “I didn’t have any self-confidence at all,” she told me. “I thought there was something wrong with me.” Claire, who was 12 at the time, also felt uncomfortable in her body in a way she couldn’t quite describe. She acknowledged that part of it had to do with puberty, but she felt it was more than the usual preteen woes. “At first, I started eating less,” she said, “but that didn’t really help.”
Around this time, Claire started watching YouTube videos made by transgender young people. She was particularly fascinated by MilesChronicles, the channel of Miles McKenna, a charismatic 22-year-old. His 1 million subscribers have followed along as he came out as a trans boy, went on testosterone, got a double mastectomy, and transformed into a happy, healthy young man. Claire had discovered the videos by accident, or rather by algorithm: They’d showed up in her “recommended” stream. They gave a name to Claire’s discomfort. She began to wonder whether she was transgender, meaning her internal gender identity didn’t match the sex she had been assigned at birth. “Maybe the reason I’m uncomfortable with my body is I’m supposed to be a guy,” she thought at the time.
Claire found in MilesChronicles and similar YouTube videos a clear solution to her unhappiness. “I just wanted to stop feeling bad, so I was like, I should just transition,” she said. In Claire’s case, the first step would be gaining access to drugs that would halt puberty; next, she would start taking testosterone to develop male secondary sex characteristics. “I thought that that was what made you feel better,” she told me.
In Claire’s mind, the plan was concrete, though neither Heather nor her husband, Mike, knew about any of it. Claire initially kept her feelings from her parents, researching steps she could take toward transitioning that wouldn’t require medical interventions, or her parents’ approval. She looked into ways to make her voice sound deeper and into binders to hide her breasts. But one day in August 2016, Mike asked her why she’d seemed so sad lately. She explained to him that she thought she was a boy.
This began what Heather recalls as a complicated time in her and her husband’s relationship with their daughter. They told Claire that they loved and supported her; they thanked her for telling them what she was feeling. But they stopped short of encouraging her to transition. “We let her completely explore this on her own,” Heather told me.
To Claire’s parents, her anguish seemed to come out of nowhere. Her childhood had been free of gender dysphoria—the clinical term for experiencing a powerful sense of disconnection from your assigned sex. They were concerned that what their daughter had self-diagnosed as dysphoria was simply the travails of puberty.
As Claire passed into her teen years, she continued to struggle with mental-health problems. Her parents found her a therapist, and while that therapist worked on Claire’s depression and anxiety—she was waking up several times a night to make sure her alarm clock was set correctly—she didn’t feel qualified to help her patient with gender dysphoria. The therapist referred the family to some nearby gender-identity clinics that offered transition services for young people.
Claire’s parents were wary of starting that process. Heather, who has a doctorate in pharmacology, had begun researching youth gender dysphoria for herself. She hoped to better understand why Claire was feeling this way and what she and Mike could do to help. Heather concluded that Claire met the clinical criteria for gender dysphoria in the DSM-5, the American Psychiatric Association’s diagnostic manual. Among other indications, her daughter clearly didn’t feel like a girl, clearly wanted a boy’s body, and was deeply distressed by these feelings. But Heather questioned whether these criteria, or much of the information she found online, told the whole story. “Psychologists know that adolescence is fraught with uncertainty and identity searching, and this isn’t even acknowledged,” she told me.
Heather said most of the resources she found for parents of a gender-dysphoric child told her that if her daughter said she was trans, she was trans. If her daughter said she needed hormones, Heather’s responsibility was to help her get on hormones. The most important thing she could do was affirm her daughter, which Heather and Mike interpreted as meaning they should agree with her declarations that she was transgender. Even if they weren’t so certain.
As heather was searching for answers, Claire’s belief that she should transition was growing stronger. For months, she had been insistent that she wanted both testosterone and “top surgery”—a double mastectomy. She repeatedly asked her parents to find her doctors who could get her started on a path to physical transition. Heather and Mike bought time by telling her they were looking but hadn’t been able to find anyone yet. “We also took her kayaking, played more board games with her and watched more TV with her, and took other short family trips,” Heather recalled. “We also took away her ability to search online but gave her Instagram as a consolation.” They told her they realized that she was in pain, but they also felt, based on what they’d learned in their research, that it was possible her feelings about her gender would change over time. They asked her to start keeping a journal, hoping it would help her explore those feelings.
Claire humored her parents, even as her frustration with them mounted. Eventually, though, something shifted. In a journal entry Claire wrote last November, she traced her realization that she wasn’t a boy to one key moment. Looking in the mirror at a time when she was trying to present in a very male way—at “my baggy, uncomfortable clothes; my damaged, short hair; and my depressed-looking face”—she found that “it didn’t make me feel any better. I was still miserable, and I still hated myself.” From there, her distress gradually began to lift. “It was kind of sudden when I thought: You know, maybe this isn’t the right answer—maybe it’s something else,” Claire told me. “But it took a while to actually set in that yes, I was definitely a girl.”
Claire believes that her feeling that she was a boy stemmed from rigid views of gender roles that she had internalized. “I think I really had it set in stone what a guy was supposed to be like and what a girl was supposed to be like. I thought that if you didn’t follow the stereotypes of a girl, you were a guy, and if you didn’t follow the stereotypes of a guy, you were a girl.” She hadn’t seen herself in the other girls in her middle-school class, who were breaking into cliques and growing more gossipy. As she got a bit older, she found girls who shared her interests, and started to feel at home in her body.
Heather thinks that if she and Mike had heeded the information they found online, Claire would have started a physical transition and regretted it later. These days, Claire is a generally happy teenager whose mental-health issues have improved markedly. She still admires people, like Miles McKenna, who benefited from transitioning. But she’s come to realize that’s just not who she happens to be.
The number of self-identifying trans people in the United States is on the rise. In June 2016, the Williams Institute at the UCLA School of Law estimated that 1.4 million adults in the U.S. identify as transgender, a near-doubling of an estimate from about a decade earlier. As of 2017, according to the institute, about 150,000 teenagers ages 13 to 17 identified as trans. The number of young people seeking clinical services appears to be growing as well. A major clinic in the United Kingdom saw a more than 300 percent increase in new referrals over the past three years. In the U.S., where youth gender clinics are somewhat newer—40 or so are scattered across the country—solid numbers are harder to come by. Anecdotally, though, clinicians are reporting large upticks in new referrals, and waiting lists can stretch to five months or longer.
The current era of gender-identity awareness has undoubtedly made life easier for many young people who feel constricted by the sometimes-oppressive nature of gender expectations. A rich new language has taken root, granting kids who might have felt alone or excluded the words they need to describe their experiences. And the advent of the internet has allowed teenagers, even ones in parts of the country where acceptance of gender nonconformity continues to come far too slowly, to find others like them.
But when it comes to the question of physical interventions, this era has also brought fraught new challenges to many parents. Where is the line between not “feeling like” a girl because society makes it difficult to be a girl and needing hormones to alleviate dysphoria that otherwise won’t go away? How can parents tell? How can they help their children gain access to the support and medical help they might need, while also keeping in mind that adolescence is, by definition, a time of fevered identity exploration?
There is no shortage of information available for parents trying to navigate this difficult terrain. If you read the bible of medical and psychiatric care for transgender people — the Standards of Care issued by the World Professional Association for Transgender Health (Wpath) — you’ll find an 11-page section called “Assessment and Treatment of Children and Adolescents With Gender Dysphoria.” It states that while some teenagers should go on hormones, that decision should be made with deliberation: “Before any physical interventions are considered for adolescents, extensive exploration of psychological, family, and social issues should be undertaken.” The American Psychological Association’s guidelines sound a similar note, explaining the benefits of hormones but also noting that “adolescents can become intensely focused on their immediate desires.” It goes on: “This intense focus on immediate needs may create challenges in assuring that adolescents are cognitively and emotionally able to make life-altering decisions.”
The leading professional organizations offer this guidance. But some clinicians are moving toward a faster process. And other resources, including those produced by major LGBTQ organizations, place the emphasis on acceptance rather than inquiry. The Human Rights Campaign’s “Transgender Children & Youth: Understanding the Basics” web page, for example, encourages parents to seek the guidance of a gender specialist. It also asserts that “being transgender is not a phase, and trying to dismiss it as such can be harmful during a time when your child most needs support and validation.” Similarly, parents who consult the pages tagged “transgender youth” on glaad’s site will find many articles about supporting young people who come out as trans but little about the complicated diagnostic and developmental questions faced by the parents of a gender-exploring child.
HRC, glaad, and like-minded advocacy groups emphasize the acceptance of trans kids for understandable reasons: For far too long, parents, as well as clinicians, denied the possibility that trans kids and teens even existed, let alone that they should be allowed to transition. Many such organizations are primarily concerned with raising awareness and correcting still-common misconceptions.
A similar motive seems to animate much of the media coverage of transgender young people. Two genres of coverage have emerged. Dating back at least to the 1993 murder of the Nebraska 21-year-old Brandon Teena, which inspired a documentary as well as the film Boys Don’t Cry, a steady stream of horror stories has centered on bullying, physical assault, and suicide—real risks that transgender and gender-nonconforming (TGNC) young people still face.
More recently, a wave of success stories has appeared. In many of these accounts, kids are lost, confused, and frustrated right up until the moment they are allowed to grow their hair out and adopt a new name, at which point they finally become their true self. Take, for example, a Parents.com article in which a mother, writing pseudonymously, explains that she struggled with her child’s gender-identity issues for years, until finally turning to a therapist, who, after a 20-minute evaluation, pronounced the child trans. Suddenly, everything clicked into place. The mother writes: “I looked at the child sitting between my husband and me, the child who was smiling, who appeared so happy, who looked as if someone finally saw him or her the way she or he saw him or herself.” In a National Geographic special issue on gender, the writer Robin Marantz Henig recounts the story of a mother who let her 4-year-old, assigned male at birth, choose a girl’s name, start using female pronouns, and attend preschool as a girl. “Almost instantly the gloom lifted,” Henig writes.
Accounts of successful transitions can help families envision a happy outcome for a suffering child. And some young people clearly experience something like what these caterpillar-to-butterfly narratives depict. They have persistent, intense gender dysphoria from a very young age, and transitioning alleviates it. “Some kids don’t waver” in their gender identity, Nate Sharon, a psychiatrist who oversaw a gender clinic in New Mexico for two and a half years, and who is himself trans, told me when we spoke in 2016. “I’m seeing an 11-year-old who at age 2 went up to his mom and said, ‘When am I going to start growing my penis? Where’s my penis?’ At 2.”
But these stories tend to elide the complexities of being a TGNC young person, or the parent of one. Some families will find a series of forking paths, and won’t always know which direction is best. Like Claire’s parents, they may be convinced that their child is in pain, but also concerned that physical transition is not the solution, at least not for a young person still in the throes of adolescence.
We are still in the earliest stages of understanding how physical transitioning affects dysphoric young people. While the specifics depend on your child’s age, and can vary from case to case, the transition process for a persistently dysphoric child typically looks something like the following. First, allow your child to transition socially: to adopt the pronouns and style of dress of their authentic gender, and to change their name if they wish. As your child approaches adolescence, get them puberty-blocking drugs, because developing the secondary sex characteristics of their assigned sex could exacerbate their gender dysphoria. When they reach their teen years, help them gain access to the cross-sex hormones that will allow them to develop secondary sex characteristics in line with their gender identity. (Until recently, hormones were typically not prescribed until age 16; it’s now more common for 15- and 14-year-olds, and sometimes even younger kids, to begin hormone therapy.)
In the United States, avoiding puberty became an option only a little more than a decade ago, so researchers have just begun tracking the kids engaged in this process, and we don’t yet have comprehensive data about their long-term outcomes. Most of the data we do have involve kids who socially transitioned at an early age, but who hadn’t yet physically transitioned. The information comes from a University of Washington researcher named Kristina Olson. Olson is the founder of the TransYouth Project, which is following a cohort of about 300 children for 20 years—the longest such longitudinal study based in the U.S. The kids she is tracking appear to be doing well—they don’t seem all that different, in terms of their mental health and general happiness, from a control group of cisgender kids (that is, kids who identify with the sex they were assigned at birth).
At the prestigious Center of Expertise on Gender Dysphoria, at Vrije Universiteit University Medical Center, in Amsterdam—often referred to simply as “the Dutch clinic”—an older cohort of kids who went through the puberty-blockers-and-cross-sex-hormones protocol was also found to be doing well: “Gender dysphoria had resolved,” according to a study of the group published in 2014 in Pediatrics. “Psychological functioning had steadily improved, and well-being was comparable to same-age peers.”
These early results, while promising, can tell us only so much. Olson’s findings come from a group of trans kids whose parents are relatively wealthy and are active in trans-support communities; they volunteered their children for the study. There are limits to how much we can extrapolate from the Dutch study as well: That group went through a comprehensive diagnostic process prior to transitioning, which included continuous access to mental-health care at a top-tier gender clinic—a process unfortunately not available to every young person who transitions.
Among the issues yet to be addressed by long-term studies are the effects of medications on young people. As Thomas Steensma, a psychologist and researcher at the Dutch clinic and a co-author of that study, explained to me, data about the potential risks of putting young people on puberty blockers are scarce. He would like to see further research into the possible effects of blockers on bone and brain development. (The potential long-term risks of cross-sex hormones aren’t well known, but are likely modest, according to Joshua Safer, one of the authors of the Endocrine Society’s “Clinical Practice Guideline” for treatment of gender dysphoria.)
Meanwhile, fundamental questions about gender dysphoria remain unanswered. Researchers still don’t know what causes it—gender identity is generally viewed as a complicated weave of biological, psychological, and sociocultural factors. In some cases, gender dysphoria may interact with mental-health conditions such as depression and anxiety, but there’s little agreement about how or why. Trauma, particularly sexual trauma, can contribute to or exacerbate dysphoria in some patients, but again, no one yet knows exactly why.
To reiterate: For many of the young people in the early studies, transitioning—socially for children, physically for adolescents and young adults—appears to have greatly alleviated their dysphoria. But it’s not the answer for everyone. Some kids are dysphoric from a very young age, but in time become comfortable with their body. Some develop dysphoria around the same time they enter puberty, but their suffering is temporary. Others end up identifying as nonbinary—that is, neither male nor female.
Ignoring the diversity of these experiences and focusing only on those who were effectively “born in the wrong body” could cause harm. That is the argument of a small but vocal group of men and women who have transitioned, only to return to their assigned sex. Many of these so-called detransitioners argue that their dysphoria was caused not by a deep-seated mismatch between their gender identity and their body but rather by mental-health problems, trauma, societal misogyny, or some combination of these and other factors. They say they were nudged toward the physical interventions of hormones or surgery by peer pressure or by clinicians who overlooked other potential explanations for their distress.
Some of these interventions are irreversible. People respond differently to cross-sex hormones, but changes in vocal pitch, body hair, and other physical characteristics, such as the development of breast tissue, can become permanent. Kids who go on puberty blockers and then on cross-sex hormones may not be able to have biological children. Surgical interventions can sometimes be reversed with further surgeries, but often with disappointing results.
The concerns of the detransitioners are echoed by a number of clinicians who work in this field, most of whom are psychologists and psychiatrists. They very much support so-called affirming care, which entails accepting and exploring a child’s statements about their gender identity in a compassionate manner. But they worry that, in an otherwise laudable effort to get TGNC young people the care they need, some members of their field are ignoring the complexity, and fluidity, of gender-identity development in young people. These colleagues are approving teenagers for hormone therapy, or even top surgery, without fully examining their mental health or the social and family influences that could be shaping their nascent sense of their gender identity.
That’s too narrow a definition of affirming care, in the view of many leading clinicians. “Affirming care does not privilege any one outcome when it comes to gender identity, but instead aims to allow exploration of gender without judgment and with a clear understanding of the risks, benefits, and alternatives to any choice along the way,” Aron Janssen, the clinical director of the Gender and Sexuality Service at Hassenfeld Children’s Hospital, in New York, told me. “Many people misinterpret affirming care as proceeding to social and medical transition in all cases without delay, but the reality is much more complex.”
…. Wpath and other organizations that provide guidance for transitioning young people call for thorough assessments of patients before they start taking blockers or hormones. This caution comes from the concerns inherent in working with young people. Adolescents change significantly and rapidly; they may view themselves and their place in the world differently at 15 than they did at 12.
“You’ve got the onset of puberty right around the age where they develop the concept of abstract thinking,” said Nate Sharon, the New Mexico psychiatrist. “So they may start to conceptualize gender concepts in a much richer, broader manner than previously—and then maybe puberty blockers or cross-sex hormones aren’t for them.” That was true for Claire: A shift in her understanding of the nature of gender led her to realize that transitioning was not the answer for her.
For younger children, gender identity is an even trickier concept. In one experiment, for example, many 3-to-5-year-olds thought that if a boy put on a dress, he became a girl. Gender clinicians sometimes encounter young children who believe they are, or want to be, another gender because of their dress or play preferences—I like rough-and-tumble play, so I must be a boy—but who don’t meet the criteria for gender dysphoria.
In the past, therapists and doctors interpreted the fluidity of gender identity among children as license to put gender-bending kids into the “right” box by encouraging—or forcing—them to play with the “right” toys and dress in the “right” clothes. Until about five years ago, according to one clinician’s estimate, social transition was often frowned upon. For decades, trans-ness was sometimes tolerated in adults as a last-ditch outcome, but in young people it was more often seen as something to be drummed out rather than explored or accepted. So-called reparative therapy has harmed and humiliated trans and gender-nonconforming children. In her book Gender Born, Gender Made, Diane Ehrensaft, the director of mental health at UC San Francisco’s Child and Adolescent Gender Center, writes that victims of these practices “become listless or agitated, long for their taken-away favorite toys and clothes, and even literally go into hiding in closets to continue playing with the verboten toys or wearing the forbidden clothes.” Such therapy is now viewed as unethical.
….
When max robinson was 17, getting a double mastectomy made perfect sense to her. In fact, it felt like her only option—like a miraculous, lifesaving procedure. Though she had a woman’s body, she was really a man. Surgery would finally offer her a chance to be herself.
I met Max, now 22, in an airy café in the quiet southern-Oregon town where she lives. She was wearing a T‑shirt with a flannel button-down over it. On her head, a gray winter cap; at her feet, a shaggy white service dog. By the time we met, we’d spoken on the phone and exchanged a number of emails, and she had told me her story—one that suggests the complexity of gender-identity development.
Max recalled that as early as age 5, she didn’t enjoy being treated like a girl. “I questioned my teachers about why I had to make an angel instead of a Santa for a Christmas craft, or why the girls’ bathroom pass had ribbons instead of soccer balls, when I played soccer and knew lots of other girls in our class who loved soccer,” she said.
She grew up a happy tomboy—until puberty. “People expect you to grow out of it” at that age, she explained, “and people start getting uncomfortable when you don’t.” Worse, “the way people treated me started getting increasingly sexualized.” She remembered one boy who, when she was 12, kept asking her to pick up his pencil so he could look down her shirt.
“I started dissociating from my body a lot more when I started going through puberty,” Max said. Her discomfort grew more internalized—less a frustration with how the world treated women and more a sense that the problem lay in her own body. She came to believe that being a woman was “something I had to control and fix.” She had tried various ways of making her discomfort abate—in seventh grade, she vacillated between “dressing like a 12-year-old boy” and wearing revealing, low-cut outfits, attempts to defy and accede to the demands the world was making of her body. But nothing could banish her feeling that womanhood wasn’t for her. She had more bad experiences with men, too: When she was 13, she had sex with an older man she was seeing; at the time, it felt consensual, but she has since realized that a 13-year-old can’t consent to sex with an 18-year-old. At 14, she witnessed a friend get molested by an adult man at a church slumber party. Around this time, Max was diagnosed with depression and generalized anxiety disorder.
In ninth grade, Max first encountered the concept of being transgender when she watched an episode of The Tyra Banks Show in which Buck Angel, a trans porn star, talked about his transition. It opened up a new world of online gender-identity exploration. She gradually decided that she needed to transition.
Max’s parents were skeptical at first but eventually came around, signing her up for sessions with a therapist who specialized in gender-identity issues. She recalled that the specialist was very open to putting her on a track toward transition, though he suggested that her discomfort could have other sources as well. Max, however, was certain that transitioning was the answer. She told me that she “refused to talk about anything other than transition.”
When Max was 16, her therapist wrote her a referral to see an endocrinologist who could help her begin the process of physical transition by prescribing male hormones. The endocrinologist was skeptical, Max said. “I think what she was seeing was a lesbian teenager,” not a trans one. At the time, though, Max interpreted the doctor’s reluctance as her “being ignorant, as her trying to hurt me.” Armed with the referral from her therapist, Max got the endocrinologist to prescribe the treatment she sought.
Max started taking testosterone. She experienced some side effects—hot flashes, memory issues—but the hormones also provided real relief. Her plan all along had been to get top surgery, too, and the initially promising effects of the hormones helped persuade her to continue on this path. When she was 17, Max, who was still dealing with major mental-health issues, was scheduled for surgery.
Because Max had parental approval, the surgeon she saw agreed to operate on her despite the fact that she was still a minor. (It’s become more common for surgeons to perform top surgeries on teenagers as young as 16 if they have parental approval. The medical norms are more conservative when it comes to bottom surgeries; Wpath says they should be performed only on adults who have been living in their gender role for at least one year.) Max went into the surgery optimistic. “I was convinced it would solve a lot of my problems,” she said, “and I hadn’t accurately named a lot of those problems yet.”
Max was initially happy with the results of her physical transformation. Before surgery, she wasn’t able to fully pass as male. After surgery, between her newly masculinized chest and the facial hair she was able to grow thanks to the hormones, she felt like she had left behind the sex she had been assigned at birth. “It felt like an accomplishment to be seen the way I wanted to be seen,” she told me.
But that feeling didn’t last. After her surgery, Max moved from her native California to Portland and threw herself into the trans scene there. It wasn’t a happy home. The clarity of identity she was seeking—and that she’d felt, temporarily, after starting hormones and undergoing surgery—never fully set in. Her discomfort didn’t go away.
Today, Max identifies as a woman. She believes that she misinterpreted her sexual orientation, as well as the effects of the misogyny and trauma she had experienced as a young person, as being about gender identity. Because of the hormone therapy, she still has facial hair and is frequently mistaken for male as a result, but she has learned to live with this: “My sense of self isn’t entirely dependent on how other people see me.”
Max is one of what appears to be a growing number of people who believe they were failed by the therapists and physicians they went to for help with their gender dysphoria. While their individual stories differ, they tend to touch on similar themes. Most began transitioning during adolescence or early adulthood. Many were on hormones for extended periods of time, causing permanent changes to their voice, appearance, or both. Some, like Max, also had surgery.
Many detransitioners feel that during the process leading up to their transition, well-meaning clinicians left unexplored their overlapping mental-health troubles or past traumas. Though Max’s therapist had tried to work on other issues with her, Max now believes she was encouraged to rush into physical transition by clinicians operating within a framework that saw it as the only way someone like her could experience relief. Despite the fact that she was a minor for much of the process, she says, her doctors more or less did as she told them.
Over the past couple of years, the detransitioner movement has become more visible. Last fall, Max told her story to The Economist’s magazine of culture and ideas, 1843. Detransitioners who previously blogged pseudonymously, largely on Tumblr, have begun writing under their real names, as well as speaking on camera in YouTube videos.
Cari Stella is the author of a blog called Guide on Raging Stars. Stella, now 24, socially transitioned at 15, started hormones at 17, got a double mastectomy at 20, and detransitioned at 22. “I’m a real-live 22-year-old woman with a scarred chest and a broken voice and a 5 o’clock shadow because I couldn’t face the idea of growing up to be a woman,” she said in a video posted in August 2016. “I was not a very emotionally stable teenager,” she told me when we spoke. Transitioning offered a “level of control over how I was being perceived.”
Carey Callahan is a 36-year-old woman living in Ohio who detransitioned after identifying as trans for four years and spending nine months on male hormones. She previously blogged under the pseudonym Maria Catt, but “came out” in a YouTube video in July 2016. She now serves as something of an older sister to a network of female, mostly younger detransitioners, about 70 of whom she has met in person; she told me she has corresponded online with an additional 300. (The detransitioners who have spoken out thus far are mostly people who were assigned female at birth. Traditionally, most new arrivals at youth gender clinics were assigned male; today, many clinics are reporting that new patients are mostly assigned female. There is no consensus explanation for the change.)
I met Carey in Columbus in March. She told me that her decision to detransition grew out of her experience working at a trans clinic in San Francisco in 2014 and 2015. “People had said often to me that when you transition, your gender dysphoria gets worse before it gets better,” she told me. “But I saw and knew so many people who were cutting themselves, starving themselves, never leaving their apartments. That made me doubt the narrative that if you make it all the way to medical transition, then it’s probably going to work out well for you.”
Carey said she met people who appeared to be grappling with severe trauma and mental illness, but were fixated on their next transition milestone, convinced thatwas the moment when they would get better. “I knew a lot of people committed to that narrative who didn’t seem to be doing well,” she recalled. Carey’s time at the clinic made her realize that testosterone hadn’t made her feel better in a sustained way either. She detransitioned, moved to Ohio, and is now calling for a more careful approach to treating gender dysphoria than what many detransitioners say they experienced themselves.
In part, that would mean clinicians adhering to guidelines like Wpath’s Standards of Care, which are nonbinding. “When I look at what the SOC describes, and then I look at my own experience and my friends’ experiences of pursuing hormones and surgery, there’s hardly any overlap between the directives of the SOC and the reality of care patients get,” Carey told me. “We didn’t discuss all the implications of medical intervention—psychological, social, physical, sexual, occupational, financial, and legal—which the SOC directs the mental-health professional to discuss. What the SOC describes and the care people get before getting cleared for hormones and surgery are miles apart.”
….
…. Within a subset of trans advocacy, however, desistance isn’t viewed as a phenomenon we’ve yet to fully understand and quantify but rather as a myth to be dispelled. Those who raise the subject of desistance are often believed to have nefarious motives—the liberal outlet ThinkProgress, for example, referred to desistance research as “the pernicious junk science stalking trans kids,” and a subgenre of articles and blog posts attempts to debunk “the desistance myth.” But the evidence that desistance occurs is overwhelming. The American Psychological Association, the Substance Abuse and Mental Health Services Administration, the Endocrine Society, and Wpath all recognize that desistance occurs. I didn’t speak with a single clinician who believes otherwise. “I’ve seen it clinically happen,” Nate Sharon said. “It’s not a myth.”
… Even some of the clinicians who have emphasized the need to be deferential to young people acknowledge the complexities at play here. A psychologist with decades of experience working with TGNC young people, Diane Ehrensaft is perhaps the most frequently quoted youth-gender clinician in the country. She is tireless in her advocacy for trans kids. “It’s the children who are now leading us,” she told The Washington Post recently. She sees this as a positive development: “If you listen to the children, you will discover their gender,” she wrote in one article. “It is not for us to tell, but for them to say.”
But when I spoke with Ehrensaft at her home in Oakland, she described many situations involving physical interventions in which her work was far more complicated than simply affirming a client’s self-diagnosis. “This is what I tell kids all the time, particularly teenagers,” she said. “Often they’re pushing for fast. I say, ‘Look, I’m old, you’re young. I go slow, you go fast. We’re going to have to work that out.’ ” Sometimes, she said, she suspects that a kid who wants hormones right now is simply reciting something he found on the internet. “It just feels wooden, is the only thing I can say,” she told me.
…Suicide is the dark undercurrent of many discussions among parents of TGNC young people. Suicide and suicidal ideation are tragically common in the transgender community. An analysis conducted by the American Foundation for Suicide Prevention and the Williams Institute, published in 2014, found that 41 percent of trans respondents had attempted suicide; 4.6 percent of the overall U.S. population report having attempted suicide at least once. While the authors note that for methodological reasons 41 percent is likely an overestimate, it still points to a scarily high figure, and other research has consistently shown that trans people have elevated rates of suicidal ideation and suicide relative to cisgender people.
But the existence of a high suicide rate among trans people—a population facing high instances of homelessness, sexual assault, and discrimination—does not imply that it is common for young people to become suicidal if they aren’t granted immediate access to puberty blockers or hormones. Parents and clinicians do need to make fraught decisions fairly quickly in certain situations. When severely dysphoric kids are approaching puberty, for instance, blockers can be a crucial tool to buy time, and sometimes there’s a genuine rush to gain access to them, particularly in light of the waiting lists at many gender clinics. But the clinicians I interviewed said they rarely encounter situations in which immediate access to hormones is the difference between suicide and survival. Leibowitz noted that a relationship with a caring therapist may itself be an important prophylactic against suicidal ideation for TGNC youth: “Often for the first time having a medical or mental-health professional tell them that they are going to take them seriously and really listen to them and hear their story often helps them feel better than they’ve ever felt.”
… When parents discuss the reasons they question their children’s desire to transition, whether in online forums or in response to a journalist’s questions, many mention “social contagion.” These parents are worried that their kids are influenced by the gender-identity exploration they’re seeing online and perhaps at school or in other social settings, rather than experiencing gender dysphoria.
Many trans advocates find the idea of social contagion silly or even offensive given the bullying, violence, and other abuse this population faces. They also point out that some parents simply might not want a trans kid—again, parental skepticism or rejection is a painfully common experience for trans young people. Michelle Forcier, a pediatrician who specializes in youth-gender issues in Rhode Island, said the trans adolescents she works with frequently tell her things like No one’s taking me seriously—my parents think this is a phase or a fad.
But some anecdotal evidence suggests that social forces can play a role in a young person’s gender questioning. “I’ve been seeing this more frequently,” Laura Edwards-Leeper wrote in an email. Her young clients talk openly about peer influence, saying things like Oh, Steve is really trans, but Rachel is just doing it for attention. Scott Padberg did exactly this when we met for lunch: He said there are kids in his school who claim to be trans but who he believes are not. “They all flaunt it around, like: ‘I’m trans, I’m trans, I’m trans,’ ” he said. “They post it on social media.”
I heard a similar story from a quirky 16-year-old theater kid who was going by the nickname Delta when we spoke. She lives outside Portland, Oregon, with her mother and father. A wave of gender-identity experimentation hit her social circle in 2013. Suddenly, it seemed, no one was cisgender anymore. Delta, who was 13 and homeschooled, soon announced to her parents that she was genderqueer, then nonbinary, and finally trans. Then she told them she wanted to go on testosterone. Her parents were skeptical, both because of the social influence they saw at work and because Delta had anxiety and depression, which they felt could be contributing to her distress. But when her mother, Jenny, sought out information, she found herself in online parenting groups where she was told that if she dragged her feet about Delta’s transition, she was potentially endangering her daughter. “Any questioning brought down the hammer on you,” she told me.
Delta’s parents took her to see Edwards-Leeper. The psychologist didn’t question her about being trans or close the door on her eventually starting hormones. Rather, she asked Delta a host of detailed questions about her life and mental health and family. Edwards-Leeper advised her to wait until she was a bit older to take steps toward a physical transition—as Delta recalled, she said something like “I acknowledge that you feel a certain way, but I think we should work on other stuff first, and then if you still feel this way later on in life, then I will help you with that.”
“Other stuff” mostly meant her problems with anxiety and depression. Edwards-Leeper told Jenny and Delta that while Delta met the clinical threshold for gender dysphoria, a deliberate approach made the most sense in light of her mental-health issues.
“At the time I was not happy that she told me that I should go and deal with mental stuff first,” Delta said, “but I’m glad that she said that, because too many people are so gung ho and just like, ‘You’re trans, just go ahead,’ even if they aren’t—and then they end up making mistakes that they can’t redo.” Delta’s gender dysphoria subsequently dissipated, though it’s unclear why. She started taking antidepressants in December, which seem to be working. I asked Delta whether she thought her mental-health problems and identity questioning were linked. “They definitely were,” she said. “Because once I actually started working on things, I got better and I didn’t want anything to do with gender labels—I was fine with just being me and not being a specific thing.”
…How best to support tgnc kids is a whiplash-inducing subject. To understand even just the small set of stories I encountered in my reporting—stories involving relatively privileged white kids with caring, involved families, none of which is necessarily the case for all TGNC young people in the United States—requires keeping several seemingly conflicting claims in mind. Some teenagers, in the years ahead, are going to rush into physically transitioning and may regret it. Other teens will be prevented from accessing hormones and will suffer great anguish as a result. Along the way, a heartbreaking number of trans and gender-nonconforming teens will be bullied and ostracized and will even end their own lives.
Some LGBTQ advocates have called for gender dysphoria to be removed from the DSM-5, arguing that its inclusion pathologizes being trans. But gender dysphoria, as science currently understands it, is a painful condition that requires treatment to be alleviated. Given the diversity of outcomes among kids who experience dysphoria at one time or another, it’s hard to imagine a system without a standardized, comprehensive diagnostic protocol, one designed to maximize good outcomes.
__________________________________
This website is educational. Materials within it are being used in accord with the Fair Use doctrine, as defined by United States law.
§107. Limitations on Exclusive Rights: Fair Use. Notwithstanding the provisions of section 106, the fair use of a copyrighted work, including such use by reproduction in copies or phone records or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use, the factors to be considered shall include: the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; the nature of the copyrighted work; the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and the effect of the use upon the potential market for or value of the copyrighted work. (added pub. l 94-553, Title I, 101, Oct 19, 1976, 90 Stat 2546)
https://www.theatlantic.com/magazine/archive/2018/07/when-a-child-says-shes-trans/561749/
Ulugh Beg
There’s a new docudrama coming out about the life of Ulugh Beg, a medieval astronomer who made Samarkand, now Uzbekistan, a thriving center of culture and science in the 15th century.
Intro adapted from Wikipedia
Mīrzā Muhammad Tāraghay bin Shāhrukh (Chagatay: میرزا محمد طارق بن شاہ رخ, Persian: میرزا محمد تراغای بن شاہ رخ), better known as Ulugh Beg (الغ بیگ) (1394- 1449), was a Timurid ruler as well as an astronomer, mathematician and sultan.
His commonly known name is a moniker, translated as “Great Ruler”
Ulugh Beg was notable for his work in astronomy-related mathematics, such as trigonometry and spherical geometry.
He built the great Ulugh Beg Observatory in Samarkand between 1424 and 1429. It is considered to have been one of the finest observatories in the Islamic world at the time. He built the Ulugh Beg Madrasah (1417–1420) in Samarkand and Bukhara, transforming the cities into cultural centers of learning in Central Asia.
He ruled Uzbekistan, Tajikistan, Turkmenistan, Kyrgyzstan, southern Kazakhstan and most of Afghanistan from 1411 to 1449.

The following is from Gizmodo, The Trailer for The Man Who Unlocked the Universe Is a Gorgeous Mixture of Science and Action, by George Dvorsky
A full 150 years before Galileo gazed at the heavens with his telescope, Ulugh Beg (1394-1449) was building some of the largest astronomical instruments on Earth. Incredibly, he used his observatory to map the stars and create charts that are still considered highly accurate, even by today’s standards.
Beg managed to measure the duration of the year to within 25 seconds of the actual figure, and he even correctly calculated the Earth’s axial tilt at 23.52 degrees. In addition to astronomy, he was a capable mathematician and biologist. He was also a Timurid ruler, transforming the cities of Samarkand and Bukhara into vibrant cultural centers.
A new 38-minute docudrama, titled Ulugh Beg: The Man Who Unlocked the Universe and directed by Bakhodir Yuldashev (Shima, Angel of Death), chronicles the life of the little-known scientist, from his birth as a prince through to his unconventional childhood and eduction, and ending with his untimely death.
Actor Armand Assante (Gotti, American Gangster) portrays Beg, and Vincent Cassel (Black Swan, Shrek) provides the narration. It features some neat CGI, live-action re-enactments of historical events, and interviews with academics and astronauts.
The film will be available for rent or purchase on Amazon starting Friday, June 22.
Bond lengths in molecules
Some people say not to use ice cubes in soda or wine because “it makes flavor molecules contract”, which supposedly makes a drink taste worse. Is this correct?
First note that flavor comes from individual molecules dissolved in solution. These are monomers, not polymers. That’s going to be important.

Let’s break the question down into two parts: Does cooling a drink make flavor molecules contract? Does cooling a drink change how our tongue perceives flavor from such molecules?
(A) Does cooling a drink make flavor molecules contract?
Let’s start with the claim that ice makes flavor molecules contract. Sounds reasonable, after all, in everyday life we see that coldness can shrink materials. For instance, a bimetallic strip consists of two different materials. Each has a different expansion coefficient (way it responds to temperature changes.) When heated, one metal expands more than the other, which forces the metal to bend. These strips are used as switches in some thermostats.

image from hyperphysics.phy-astr.gsu.edu
More commonly, we see large scale materials contract when cooled, like highways. That is why roads over bridges, and in parking lots, need thermal expansion joints. Otherwise the shrinking and expansions would otherwise break the surface.

image from Ontario Ministry of Transportation, Bridge Repairs
Characterization of Typical Potent Odorants in Cola-Flavored Carbonated Beverages
Molecules in Coca Cola (Compound Interest)
Molecules in wine (Compound Interest)
Molecules in whiskey (Compound Interest)
But why do these materials contract when cooled? Has each individual molecule shrunk? No. To understand why we need to think about intermolecular vs intramolecular forces.
Intermolecular forces hold one molecule to another.

image from dynamicscience.com.au
Intramolecular forces hold atoms together within a single molecule. (e.g. chemical bonds, covalent bonds)

The naming comes from Latin roots
inter meaning between or among
intra meaning inside
When we use ice to cool a drink from 75 F down to 45 F, does the size of an individual molecule change in any appreciable way? Well, as we see here, a heated molecule can vibrate faster or slower – but the distance between atoms doesn’t appreciably change: the size of any single molecule is constant.

Nope. First, notice that the temperature in either F or C is misleading. Those temperatures are only measured relative to the freezing point of water. A better comparison is comparing their absolute temperature using the Kelvin scale
75 F = 24 C = 297 K
45 F = 7 C = 280 K
Wow, on an absolute scale this doesn’t change the temperature of the molecules very much.
Now sure, cooling does reduce molecular vibration: this allows intermolecular forces to pull the molecules closer together, which causes shrinking of the material as a whole. Still, this doesn’t change the bond lengths within a molecule.
(B) Does cooling a drink change how our tongue perceives flavor from such molecules?
If flavor change exists then I would think it is because the tongue tastes certain molecules better at certain temperatures.

image from blogs.unimelb.edu.au, The University of Melbourne, Scientific Scribbles, Let’s talk about Taste
images
https://maxfacts.uk/help/oral-food/ttt
discussion
https://www.ncbi.nlm.nih.gov/books/NBK236241/
https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072592/
https://www.livescience.com/20286-foods-taste-hot-cold.html
https://academic.oup.com/chemse/article/42/2/153/2547704
https://www.beveragedaily.com/Article/2005/12/19/Food-temperature-affects-taste-reveal-scientists
https://www.quora.com/How-exactly-does-temperature-affect-the-taste-of-food-and-beverages
Learning Standards
Next Generation Science Standards
HS-PS1-3. Plan and conduct an investigation to gather evidence to compare the structure of substances at the bulk scale to infer the strength of electrical forces between particles. The structure and interactions of matter at the bulk scale are determined by electrical forces within and between atoms.
Massachusetts Science and Technology/Engineering Curriculum Framework
HS-PS1-3. Cite evidence to relate physical properties of substances at the bulk scale to spatial arrangements, movement, and strength of electrostatic forces among ions, small
molecules, or regions of large molecules in the substances. Make arguments to
account for how compositional and structural differences in molecules result in
different types of intermolecular or intramolecular interactions.
Common Core State Standards Connections:
Sea level rise
Should we be worried about surging Antarctic ice melt and sea level rise?
Dana Nuccitelli, The Guardian, 18 Jun 2018
There’s recently been a spate of sea level rise denial in the conservative media, but in reality, sea level rise is accelerating and melting ice is playing an increasingly large role. In the first half of the 20th Century, average global sea level rose by about 1.4 millimeters per year (mm/yr). Since 1993, that rate has more than doubled to 3.2 mm/yr. And since 2012, it’s jumped to 4.5 mm/yr.

Global mean sea level data from the Colorado University Sea Level Research Group, with 4-to-5-year linear trends shown in black and red. Illustration: Dana Nuccitelli
Thermal expansion (ocean water expanding as it warms) continues to play the biggest role in sea level rise, but its contribution of about 1.3 mm/yr is now responsible for a smaller proportion of total sea level rise (30% in recent years) than its contribution since the 1990s (40% of the total). That’s because of the acceleration in melting ice.
Glacier melt is accelerating, recently contributing about 0.75 mm/yr to sea level rise, up from 0.65 mm/yr since the 1990s. But the biggest jumps have come from ice in Greenland and Antarctica. Greenland had been responsible for about 0.48 mm/yr sea level rise since 1990, but in recent years is up to 0.78 mm/yr. A recent study in Nature Climate Change found that Greenland contributed about 5% to sea level rise in 1993 and 25% in 2014.
Antarctica is a huge question mark with warning signs
A new study published in Nature using data from a range of satellites found that Antarctica’s contribution has tripled from about 0.2 mm/yr since the 1990s to 0.6 mm/yr since 2012, during which time global sea level rise also spiked. Accelerated ice melt from Antarctica, Greenland, and glaciers have all played a role in the faster recent sea level rise. The question is whether it’s a temporary jump, or if we need to worry about a continued acceleration in Antarctic ice loss.
Another recent paper published in Earth’s Future found that rapid losses from Antarctic ice are plausible. The study found that in moderate to high carbon-emission scenarios, an average expected sea level rise of 2 to 2.5 feet by 2100 could actually become 3 to 5 feet once Antarctic ice sheet dynamics are taken into account.
The vast majority of Antarctica’s current ice loss is coming from West Antarctica, where about 75% of the glaciers are located below sea level. In East Antarctica, which has so far remained stable, only about 35% of the glaciers are below sea level. Warming ocean waters are melting the Antarctic ice from below, which is particularly problematic for that low-lying ice in West Antarctica. Research suggests that the collapse of the Western Antarctic ice sheet is already unstoppable.

The amount of ice loss across Antarctica in total (purple), and in West Antarctica (green), East Antarctica (yellow) and the Antarctic Peninsula (red). Illustration: Shepherd et al. (2018), Nature
Should we be worried?
Short term variations in sea level rise do happen. Sea level actually briefly fell in 2010 due to a strong La Niña cycle, which typically results in an increase of rain and snow falling over land. This resulted in a number of epic deluges and flooding across the globe; more water on land temporarily meant less in the ocean.
However, Antarctica and Greenland could potentially cause rapid sea level rise. As James Hansen explains in the video below, there have been periods in the not-so-distant past when sea levels rose at an average rate of 1 meter every 20 years.
In past eras when temperatures and atmospheric carbon dioxide levels were similar to those today and to the Paris climate targets, like in the last interglaciation and the Pliocene, sea levels were about 20 to 80 feet higher. Unless we manage to actually cool global temperatures, we’re certainly due for significantly more sea level rise. The large ice sheets on Greenland and Antarctica will continue to melt for as long as 1,000 years. That’s why sea levels were so much higher in past eras whose climates remained at hot temperatures like today’s for thousands of years.
It takes time for ice to melt. The question is, how fast will it happen? Sea level rise unquestionably poses a long-term threat, but how much of a short-term threat largely depends on just how stable the Antarctic ice sheet turns out to be. The recent acceleration of Antarctic ice loss, while not yet definitive, is certainly cause for concern.
________________________________
This website is educational. Materials within it are being used in accord with the Fair Use doctrine, as defined by United States law.
§107. Limitations on Exclusive Rights: Fair Use. Notwithstanding the provisions of section 106, the fair use of a copyrighted work, including such use by reproduction in copies or phone records or by any other means specified by that section, for purposes such as criticism, comment, news reporting, teaching (including multiple copies for classroom use), scholarship, or research, is not an infringement of copyright. In determining whether the use made of a work in any particular case is a fair use, the factors to be considered shall include: the purpose and character of the use, including whether such use is of a commercial nature or is for nonprofit educational purposes; the nature of the copyrighted work; the amount and substantiality of the portion used in relation to the copyrighted work as a whole; and the effect of the use upon the potential market for or value of the copyrighted work. (added pub. l 94-553, Title I, 101, Oct 19, 1976, 90 Stat 2546)
Dinosaurs
What is a dinosaur?
There’s a big difference between what people think a dinosaur is, and what a dinosaur actually is.
Many people would identify the dimetrodon (left) as a dinosaur and the deinonychus (right) as a non-dinosaur, more specifically they might identify it as a bird.
And yet both would be wrong:


Dimetrodons lived 40 million years before dinosaurs even existed – and they are more closely related to mammals than to dinosaurs.
While the deinonychus, on the right, is a dinosaur.
What about all those other animals that people think of as dinosaurs?
Pterosaurs? Also called pterodactyls. Not a dinosaur. A flying reptile.

Mosasaurs? Not a dinosaur. They are an extinct group of aquatic lizards.

Image from NPS website, Thomas Miller (c) / Badlands Natural History Association
Mosasaur: Apex Predator of the Western Interior Seaway, NPS
Ichthyosaurs? Not a dinosaur. Marine reptile

Plesiosaurs? Not a dinosaur. Mesozoic marine reptiles.

Restored skeleton of Plesiosaurus. Photo by Kim Alaniz via Wikipedia.
Dimetrodon? Not a dinosaur.
All of the various dimetrodon species became extinct 40 million years before the first appearance of dinosaurs.
They are reptile-like in appearance and physiology, yet nevertheless they are more closely related to mammals than to modern reptiles!
To be clear, they are not a direct ancestor of mammals; they were sort of a cousin branch to the mammals.

Most of those aren’t dinos? How can common beliefs be so incorrect?
People think that dinosaurs are a very specific thing – something related to images from popular movies and children’s books. Yet in reality dinosaurs are just as varied as mammals.
Consider: Which of the following are mammals? All of them!
They’re an incredibly varied class of animals. Yet they all form one clade on the evolutionary tree of life.

from exploringnature.org/db/view/Class-Mammals-4th-Grade-and-up
Turns out that the same is true for dinosaurs: they’re an incredibly varied class of animals – yet at the same they all form one clade on the evolutionary tree of life.
They have some characteristics in common.

from Encyclopedia Britannica
Origin of the dinosaurs
Their ancestors were archosaurs, egg-laying reptiles.
They began to develop as a distinct group around 250 MYA (million years ago.)

On a related note see
The Forgotten Archosaurs
The “Dinosaurs” that Weren’t: The [brief] Age of Pseudosuchians
Pseudosuchian archosaurs, National Park Arizona
Archosaurs have two holes (temporal fenestra) in each side of their skulls. These reduce the weight of the skull.

Over time Archosaurs split into several groups: Let’s go through this cladogram carefully. The far past is in the bottom, and as we read upwards we move forward in time.

from GEOL 104 Dinosaurs: A Natural History
Let’s look carefully at this family tree: Where are the crocodiles? pterosaurs? Dinosaurs?
Where are the Silesauridae? (They are the sister group of dinosaurs)
What are pterosaurs?
What are crocodilia (crocodilians)?
These include crocodiles, alligators, caimans, and gharials.

What are the actual dinosaurs?
Dinosaurs are the branch descended from archosaurs that have hind limbs held erect beneath the body.
It is their hip structure that most obviously distinguishes dinosaurs from other related groups.
Because of their hips, many dinosaurs could have an upright, bipedal way of walking (like today’s birds.)
Some dinosaurs were quadrupeds (usually walking on all fours) but they were still capable of standing up on their hind legs.
Also see About Sauropod Dinosaurs

See how dinosaurs have hips that allow them to stand? Reptiles can’t do this. Image from Jurassic Park.
Compare this today’s turtles, lizards and crocs – their legs splay out beneath them.
This is clear when we look at the differences between the far left and far right images:

Image from dinosaurjungle.com
Types of dinosaurs
saurischians (‘lizard hipped dinosaurs’) and ornithischians (‘bird hipped dinosaurs’)
For the sake of convenience, the dinosaur family is divided into two main groups.
About 230 million years ago a subgroup of archosaurs split off into two types of dinosaurs, distinguished by the structure of their hip bones.
Saurischian (“lizard-hipped”) dinosaurs went on to include predators like Tyrannosaurus Rex and huge sauropods like Apatosaurus

Images from Saurischia, Wikipedia
Ornithischian (“bird-hipped”) dinosaurs consisted of a diverse assortment of other plant eaters, including hadrosaurs, ornithopods and stegosaurs.

Images from Saurischia, Wikipedia
Confusingly, we now know that birds descended from “lizard-hipped,” rather than “bird-hipped,” dinosaurs.
Learn more about how are dinosaurs classified here:
What Is the Scientific Definition of a Dinosaur, According to Experts?
What Makes a Dinosaur a Dinosaur? Smithsonian magazine

CC BY-SA 3.0, Wikipedia, Evolution of dinosaurs, Zureks
Possible new way of classifying dinosaurs
Honors level. These details are for students interested in the latest understanding of evolution.
http://www.drneurosaurus.com/2017/03/a-new-dinosaur-family-tree/
Ornithoscelida Rises: A New Family Tree for Dinosaurs, Scientific American
Discussion from Carnivoraforum
How did birds evolve from dinosaurs?
Short version: Almost all branches of the dinosaur family tree died out, except for the branch with small feathered dinosaurs. That branch proliferated and developed into the birds that we know today.

Image by Shawn Gould and Jen Christiansen, from How Dinosaurs Grew So Large—And So Small John R. Horner, Kevin Padian and Armand de RicqlèS Scientific American 293, 56 – 63 (2005)
and

Zina Deretsky, National Science Foundation. Air sac system of birds and of Majungasaurus.
also see The origin of birds evolution.berkeley.edu
How did most dinosaurs become extinct?
Short version: Meteor impact – and perhaps associated Deccan traps volcanic event? See Meteor impacts on Earth
How do we learn about dinosaurs? Fossils
See Dating rocks and fossils
and also Geologic eras
The science of Jurassic Park
Jurassic Park is a 1993 film directed by Steven Spielberg. The first installment of the Jurassic Park franchise, it is based on the 1990 novel of the same name by Michael Crichton. Is there any basis to the science in this movie?
The science of Jurassic Park
Mythology and dinosaurs
How some mythology was inspired by finding fossils
Dinosaurs and their role in mythology
Reptiles are not a true clade
Section TBA
There’s No Such Thing As Reptiles Any More – And Here’s Why
Learning Standards
Next Generation Science Standards
HS-LS4-1. Communicate scientific information that common ancestry and biological evolution are supported by multiple lines of empirical evidence.
HS-LS4-1. Communicate scientific information that common ancestry and biological evolution are supported by multiple lines of empirical evidence.
HS-LS4-2. Construct an explanation based on evidence that the process of evolution primarily results from four factors: (1) the potential for a species to increase in number, (2) the heritable genetic variation of individuals in a species due to mutation and sexual reproduction, (3) competition for limited resources, and (4) the proliferation of those organisms that are better able to survive and reproduce in the environment.
HS-LS4-3. Apply concepts of statistics and probability to support explanations that organisms with an advantageous heritable trait tend to increase in proportion to organisms lacking this trait.
HS-LS4-4. Construct an explanation based on evidence for how natural selection leads to adaptation of populations.
HS-LS4-5. Evaluate the evidence supporting claims that changes in environmental conditions may result in (1) increases in the number of individuals of some species, (2) the emergence of new species over time, and (3) the extinction of other species.
MCAS Open response
Sarah and her biological sister Danielle have some physical characteristics that are the same and some that are different, as shown in the table below.

a. Identify the molecule that stores the hereditary information for these characteristics in the chromosomes of every body cell.
b. Identify the total number of chromosomes that should be in one of Sarah’s body cells and the number of chromosomes that should have been contributed by each biological parent.
c. Explain the roles of meiosis and fertilization in achieving the chromosome numbers you identified in part (b).
d. Explain why Sarah and Danielle have some physical characteristics that are different from each other, even though they have the same biological parents.
See
Ferris wheel physics
A Ferris wheel is a large structure consisting of a rotating upright wheel, with multiple passenger cars.
The cars are attached to the rim in such a way that as the wheel turns, they are kept upright by gravity.

The original Ferris Wheel was designed and constructed by George Washington Gale Ferris Jr. as a landmark for the 1893 World’s Columbian Exposition in Chicago.
The generic term Ferris wheel is now used for all such structures, which have become the most common type of amusement ride at state fairs in the United States.
Forces in the wheel
The wheel keeps its circular shape by the tension of the spokes, pulling upward against the lower half of the framework and downward against the huge axle.
Also see
Classical relativity
This animation shows simultaneous views of a ball tossed up and then caught by a ferris wheel rider –
It shows this from one inertial POV and from two non-inertial POVs.
P. Fraundorf writes
Although Newton’s predictions are easier to track from the inertial point of view, it turns out that they still work locally in accelerated frames and curved spacetime if we consider “geometric accelerations and forces” that act on every ounce of an object’s being and can be made to disappear by a suitable vantage point change.

Created by P. Fraundorf, licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license.
Net work done on you while on the wheel
if you are on a ferris wheel that is rotating, the total work done by all the forces acting on your is zero.
https://www.physicsforums.com/threads/ferris-wheel-work-done-by-net-force.715905/
External resources
https://www.real-world-physics-problems.com/ferris-wheel-physics.html
https://physics.stackexchange.com/questions/205918/centripetal-force-on-a-ferris-wheel
How products are made: http://www.madehow.com/Volume-6/Ferris-Wheel.html
AP Physics problems: Ferris wheels and rotational motion
Build A Big Wheel, by Try Engineering, Lesson plan
AP Physics problem solving
http://faculty.washington.edu/boynton/114AWinter08/LectureNotes/Le8.pdf
PHYSICS IN THE EXPANSE
The Expanse is a series of science fiction novels, novellas and stories by James S. A. Corey – the pen name of authors Daniel Abraham and Ty Franck. The first novel, Leviathan Wakes, was nominated for the Hugo Award for Best Novel in 2012. In 2017 the series as a whole was nominated for the ‘Best Series’ Hugo Award.
These novels are the basis of an American science fiction television series developed by Mark Fergus and Hawk Ostby. The series received positive reviews from critics, who highlighted its visuals, character development, and political narrative. It received a Hugo Award for Best Dramatic Presentation as well as a Saturn Award nomination.
- Wikipedia

https://nerdist.com/getting-the-science-right-makes-the-expanse-a-better-show/
https://www.wired.com/story/the-physics-of-accelerating-spacecraft-in-the-expanse/
https://www.reddit.com/r/TheExpanse/comments/434ihh/what_kind_of_physics_is_the_epstein_drive_based/
LET’S DO THE PHYSICS OF KNOCKING AN ASTEROID INTO THE SUN, Rhett Allain
http://josephshoer.com/blog/2015/06/spaceships-of-the-expanse/
Books
Main article: The Expanse (novel series)
-
Leviathan Wakes (June 15, 2011)
-
Caliban’s War (June 26, 2012)
-
Abaddon’s Gate (June 4, 2013)
-
Cibola Burn, (June 5, 2014)
-
Nemesis Games (June 2, 2015)
-
Babylon’s Ashes (December 6, 2016)
-
Persepolis Rising (December 5, 2017)
-
Tiamat’s Wrath (December, 2018)
Related works
-
“The Butcher of Anderson Station” (The Expanse short story) (2011)
-
Gods of Risk (The Expanse novella) (2012)
-
“Drive” (The Expanse short story) (2012)
-
The Churn (The Expanse novella) (2014)
-
The Vital Abyss (The Expanse novella) (2015)
-
Strange Dogs (The Expanse novella) (2017)
Television series
tba
Possible rocket engines
from ATOMIC ROCKETSHIPS OF THE SPACE PATROL or “So You Wanna Build A Rocket?” by Winchell D. Chung Jr..
Here is your handy-dandy cheat-sheet of rocket engines. Use this as a jumping-off point, there is no way I can keep this up-to-date. Google is your friend!
I’ll point out a few of the more useful items on the sheet:
-
Aluminum-Oxygen is feeble, but is great for a lunar base (the raw materials are in the dirt).
-
VASIMR is the current favorite among ion-drive fans. Use this with orbit-to-orbit ships that never land on a planet. It can “shift gears” like an automobile.
-
Solar Moth might be a good emergency back-up engine.
-
Nuclear Thermal Solid Core is better than feeble chemical rockets, but not as much as you’d expect.
-
Nuclear Thermal Vapor Core is what you design along the way while learning how to make a gas core atomic rocket.
-
Nuclear Thermal Gas Core Open-Cycle is a full-blown honest-to-Heinlein atomic rocket, spraying glowing radioactive death in its exhaust.
-
Nuclear Thermal Gas Core Closed-Cycle is an attempt to have the advantages of both nuclear solid core and gas core, but often has the disadvantages of both. It has about half the exhaust velocity of an open-cycle atomic rocket.
-
Orion Nuclear Pulse is a rocket driven by detonating hundreds of nuclear bombs. If you can get past freaking out about the “bomb” part, it actually has many advantages. Don’t miss the Medusa variant.
-
Magneto Inertial Fusion This is the best fusion-power rocket design to date.
-
Zubrin’s Nuclear Salt Water This is the most over-the-top rocket. Imagine a continuously detonating Orion drive. There are many scientist who question how the rocket can possibly survive turning the drive on.
Latest Posts
-

Importance of art education
Why is teaching art intrinsically important to being human? Some would have us believe that we should have art education in our schools because it…
-

What are broken symmetries?
Symmetry is an important concept for understanding how our universe works. Symmetry lets us see what stays the same when certain conditions change. Symmetries are…
-

Native Americans in New England
When did the ancestors of native Americans arrive in what we now call New England? Their earliest confirmed presence in New England is about 12,000–13,000…
-
Why is music education important
Why is music intrinsically important to being human? Every year I read yet another article trying to persuade us that we should have music education…

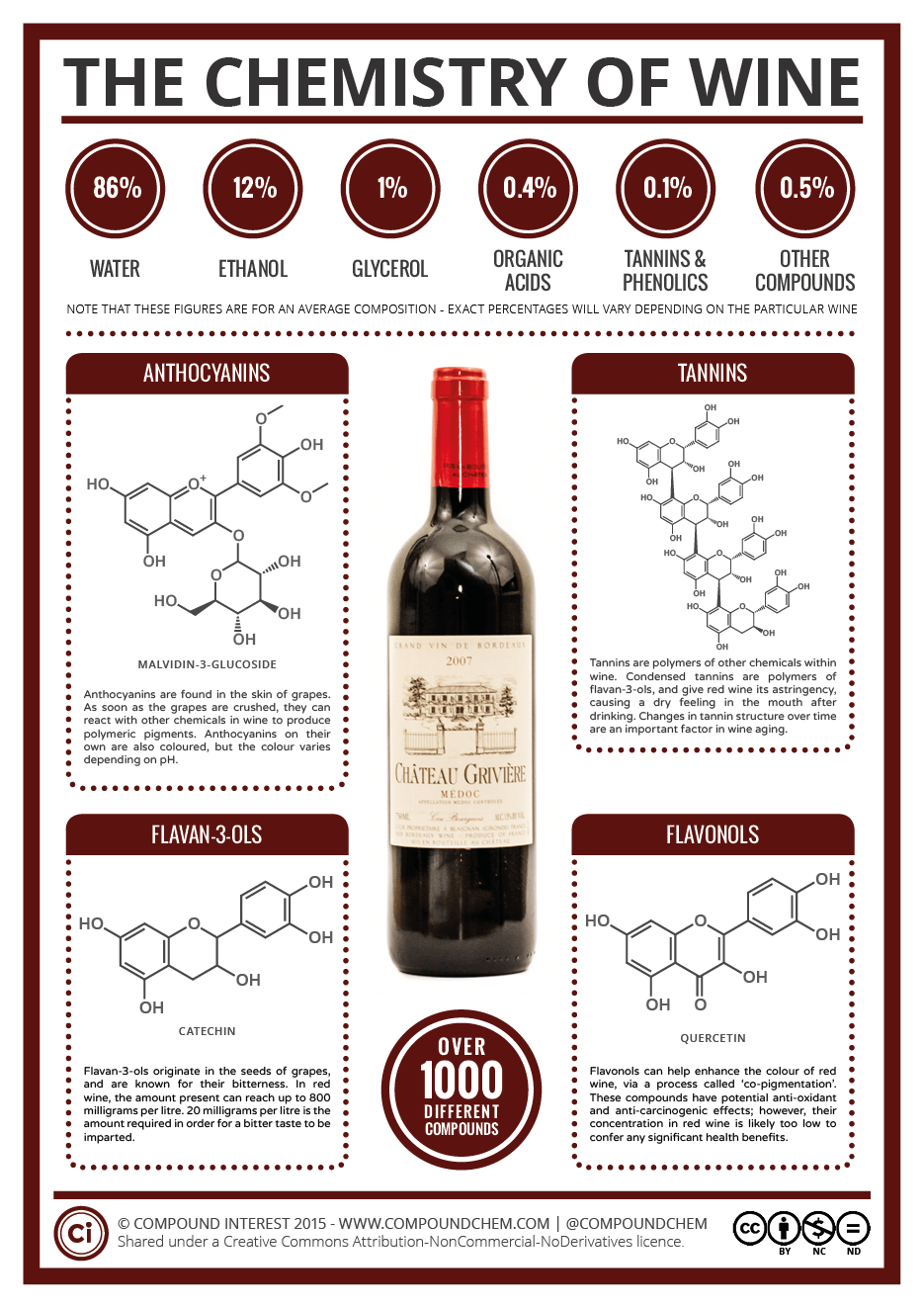{kind=link}